Transcatheter Aortic Valve Implantation (TAVI)
The heart is a muscle which pumps blood to your lungs and around the body. There are four valves within the heart. These valves normally open to let blood flow through, or out, of the heart, and then shut to prevent blood flowing backwards. If a valve becomes diseased or damaged this can affect the flow of blood in two ways: 1. If the valve does not open fully it will obstruct the flow. This is called valve stenosis. 2. If the valve does not close properly it will allow blood to flow backwards in the wrong direction. This is called valve regurgitation.
“My utmost priority is to provide the highest quality and most up-to-date cardiovascular care to all my patients. I aim to achieve this using a holistic approach in a personable and empathetic atmosphere, while taking into consideration each individual patient’s own wishes and hopes for their medical care.”
Aortic valve stenosis
The aortic valve is on the left side of the heart. When the valve opens blood is normally pumped from the left chamber of the heart (ventricle) around the body. When the aortic valve is narrowed the blood flow out of the heart is restricted. This is known as aortic stenosis. This can cause symptoms of chest pain, breathlessness and/ or dizziness when exercising, and can lead to fainting. The restriction may also put a strain onto your heart pump, leading to heart muscle weakness, fluid in the lungs or swollen ankles. The preferred treatment for severe symptomatic aortic valve stenosis in the past was conventional aortic valve replacement. This involves open-heart surgery to replace the narrowed valve with a new artificial one. However, your doctor will determine whether you may be suitable for a less invasive transcatheter aortic valve implantation.
More Details
What is Transcatheter Aortic Valve Implantation?
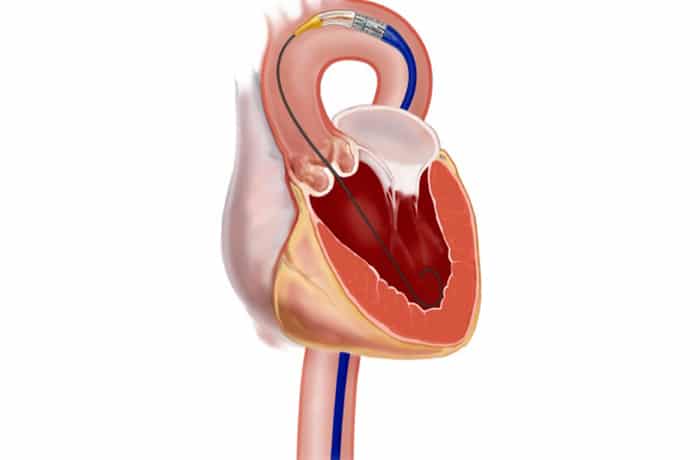
Transcatheter aortic valve implantation (TAVI) involves inserting a new artificial heart valve inside the old tight valve using a balloon catheter. The valve is made up of a metal frame (stent) and the outer lining (pericardium) of a cow’s or a pig’s heart. The procedure can be carried out under either general anaesthetic or local anaesthetic with or without conscious sedation.
The main route of new valve insertion is through the femoral artery, the main artery in your groin which leads back to the heart (Transfemoral Route). In rare cases, an alternative access route is used through a small cut on the left side of your chest to get to the apex (tip) of your heart (Transapical Route). The ‘TAVI team’, including your cardiologist, cardiac surgeon and anaesthetist will review your medical condition and screening tests to decide the most appropriate treatment and access route for you.
What screening tests will be performed prior to the procedure?
- Physical examination
- An electrocardiogram (ECG)
- A chest X-ray (CXR)
- Blood tests
- An ultrasound probe and gel placed on the chest to obtain pictures of your heart (transthoracic echocardiogram)
- Possibly a transoesophageal echocardiogram (TOE) if clearer pictures are needed (this involves swallowing an ultrasound probe under sedation)
- A coronary angiogram, which involves passing a tube (catheter) into your groin or wrist artery and taking X-ray pictures of your blood vessels supplying your heart (coronary arteries), your body’s main blood vessel (aorta) and groin arteries.
- CT scan
Hospital admission
Once accepted by the medical team, and the funding for your operation is available, you will be invited in for the operation. You will receive a letter with your admission details. This will usually ask you to stop any blood thinning medications 2 to 5 days before your operation (depending on the type of blood thinner). You will be asked to come in the day before your procedure for preparation. Before the operation, you will be seen by members of the operating team. You will be kept ‘nil by mouth’ for a few hours prior to your procedure and the nurses will assist you to shave your chest, wrists and groins and also to shower. The procedure will be done in the catheterization laboratory (similar room to where you had the coronary angiogram) using contrast dye to guide the valve into the correct position.
Procedure
You will be given a local anaesthetic and conscious sedation and have a drip inserted into your neck and arm. If a general anaesthetic is used, you will also have a urinary catheter inserted into your bladder. You will have some tubes put through the blood vessels in your groin to deliver the contrast dye and a pacing wire to speed up the heart during the valve insertion to ensure correct positioning. The cardiologist will gain access making a small incision either in your groin. A catheter (narrow tube) is passed from the femoral (groin) artery to the aorta (transfemoral). The catheter allows a balloon to be placed into your tight valve, the balloon is inflated to stretch the valve open. This part of the procedure is called balloon aortic valvuloplasty (BAV). The new valve for implantation will be carefully compressed and mounted onto a balloon delivery catheter. When the valve is in the correct position your heart rate will be increased using the temporary pacing wire for a few seconds. This reduces the blood pressure and the motion of the heart making the procedure safer. The balloon is then expanded opening up the replacement valve in to a permanent position. The balloon is deflated and removed leaving the new valve to function immediately. Once the catheters are removed at the end of the procedure the blood vessel in the groin is closed using a vascular closure device. The procedure takes one to two hours. Following your procedure you will go from the catheterization laboratory to the recovery area for several hours where you will be closely monitored. Following this you will return either to the ward or the high dependency unit. If a general anaesthetic was used you will be normally woken up early after the operation but occasionally you may need to stay asleep so will be kept sedated and if necessary admitted to intensive care. Over the next 24 hours you will have your drips removed. You will be in hospital for up to five days depending on how quickly you recover.
Potential benefits of a TAVI procedure
Treatment with the new valve should improve your symptoms. It will give you a more normal aortic valve performance and improve your overall heart function. We would hope this will increase your life expectancy and improve your quality of life.
Potential risks of a TAVI procedure
- Risk of heart attack: 1%
- Risk of stroke: 2-3%
- Risk of death during the procedure approximately: 2%
- Risk of requiring a permanent pacemaker: 3%
- Damage to groin arteries
- Bleeding
- Infection
- Kidney failure (if impaired kidney function existed prior to surgery)
- Emergency open heart surgery 0.5%
Recovery at home
The following are only general guidelines as everyone’s recovery is slightly different. It is advisable that you have someone to care for you for the first week after discharge. Please speak to your nurse or doctor as soon as possible if you think this will be a problem.
Activity
You should avoid strenuous activity for 2-3 weeks. This includes heavy lifting (eg shopping, suitcases) or pushing and pulling (eg cutting grass, vacuum cleaning). You may feel a little ‘washed out’ and tired and need to rest in the afternoon. However it is important for your recovery to have a short walk every day. This can be gradually increased. You do not have to avoid climbing stairs or walking up inclines, you may have to start off at a slower pace. You may feel slightly out of breath on walking, which should improve as your fitness level increases. There can be some fluid retention as a result of the surgery; you may notice some swelling of your ankles. If this swelling travels further than your ankles please get reviewed by your GP.
Wounds
Your wounds should be healed by the time you leave hospital, if they still require a dressing we will organise a District or practice nurse to continue this. The stitches are dissolvable so do not have to be removed. If your wound becomes red or inflamed please get your GP or practice nurse to check it. You may have bruising to your groin(s) which is not uncommon and may take several weeks to resolve. You may have a hard lump under the skin due to a collection of blood (haematoma). Please consult your GP if this becomes painful or grows bigger.
Medication
As well as your normal medicines including aspirin, you will usually be discharged with an additional blood thinning medicine called clopidogrel. This will be required for at least three months. After this you will only need to take the aspirin. People on warfarin or Novel Oral Anticoagulants (NOAC) may only require and addional aspirin or clopidogrel. You will be discharged with some painkillers, which we would recommend you to take regularly until you are no longer getting discomfort from your wound.
Driving
You are not allowed to drive for four weeks after your procedure. If you have a LGV or PCV licence you will need to undergo an exercise test before getting your licence back.
Work
If you were working before your procedure there is no reason why you cannot return to this after a period of recovery up to 4 weeks.
Cardiac rehabilitation
You will be invited to attend cardiac rehabilitation about six weeks after your procedure. This is a programme of graduated exercise and general health discussions. If you live outside the Cork area you may be referred to your local hospital. Patients who attend generally feel more confident about coping with everyday life. It will also help to increase your fitness level.
Follow-up care
On discharge you will be given a letter for your G.P explaining what you have had done and a list of your medications. The cardiac nurse will phone you a week or so after discharge to check on your progress. If you have any concerns you can call the Cardiac Nurse on 021 454 2807 bleep 122 (Monday to Thursday 07.30 – 18.00; Friday 07:30-13:00). We would like to hear sooner rather than later about any potential problems. You will be invited to attend an outpatient follow up appointment about six weeks after your procedure. During this visit you will have an echo. The doctor will then decide about any future appointments.
How to contact us
If you need further information please contact Mary Connor or Anne Dowling, Cardiac Nurses, on 021 4542807 Bleep 122.










